
TST 2016, Hua Hin, Thailand 2016/03/16-18
Modification of skin redraping method for medial epicanthoplasty
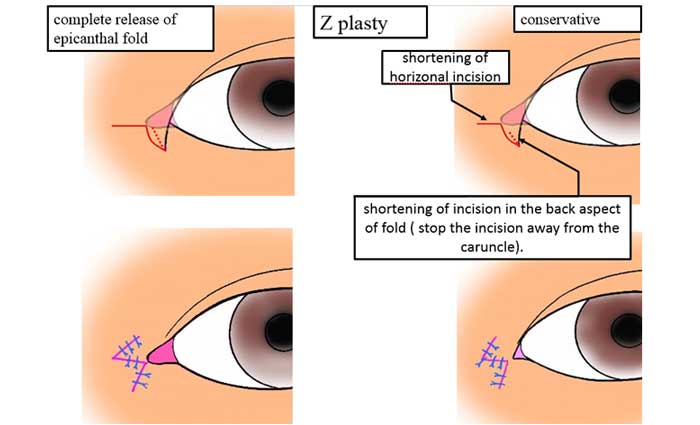
In OSAPS 2014 in Pattaya,I presented the comparison study of epicanthoplsty between Park’s root Z plasty and Dr.Oh’s skin redraping method.
The study showed that the vertical scar of Z plasty was visible and annoying to not a few patients.
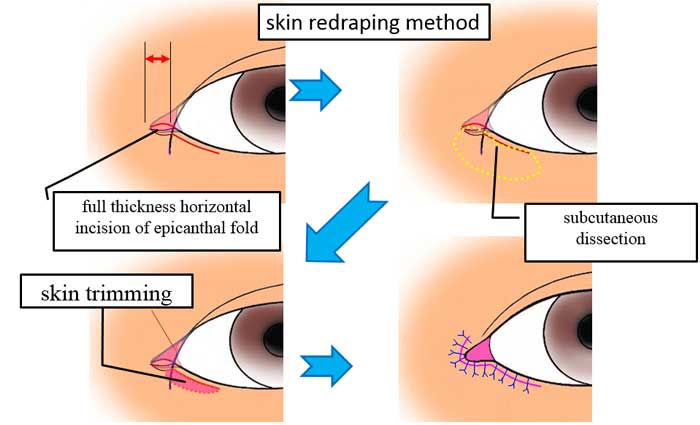
The skin redraping method made a scar in the less visible area than the Z plasty.
The redraping has smaller effect to release the vertical skin tension of the epicanthal fold; therefore, this method tends to create in-fold type of double fold.
The redraping method requires the trimming of lower eyelid skin; this maneuver had a potential risk for unfavorable downward expansion of the caruncle.
Since 2011, I have used modified method of skin redraping.
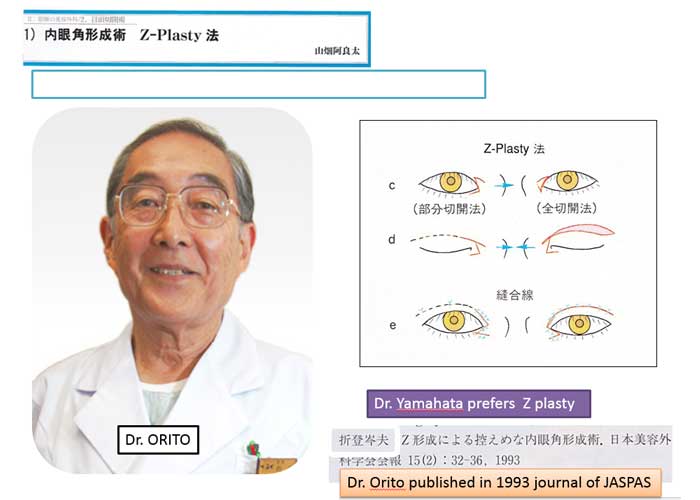
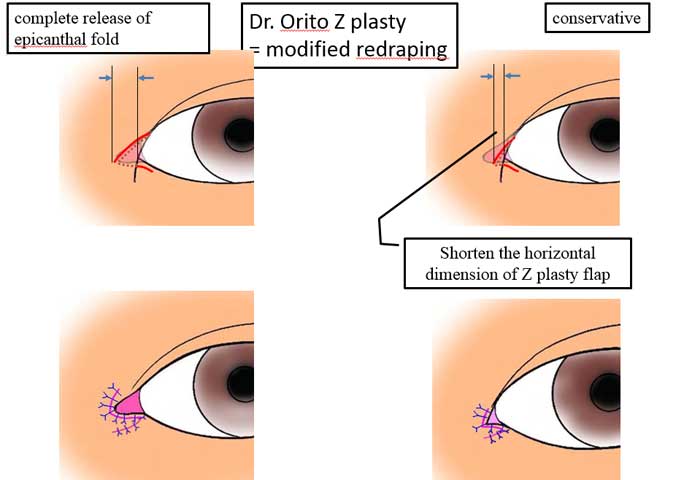
This procedure utilizes Z plasty presented by Japanese plastic surgeon, Dr. Orito in 1993.
The resultant scar is in L shaped, which is similar to that of skin redraping.
This modified method is more effective to release the vertical tension in the medial canthal region.
The technical details and clinical results will be demonstrated in this paper.
Summary presented in OSAPS 2014
・The redraping has smaller effect to release the vertical skin tension ; therefore, there is a chance of creating in-fold line after redraping
・The Z plasty is more reliable for creating out-fold line.

Reconstruction of Mongolian fold for revision epicanthoplasty
The epicanthoplasty is a common procedure in Oriental blepharoplasty.
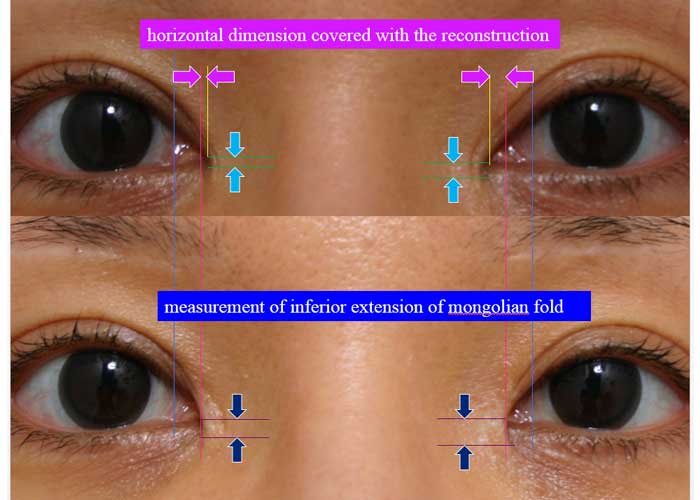
Over-show of caruncle can cause patients’ dissatisfaction.
This paper presents my clinical experiences of reconstructing the epicanthal fold.
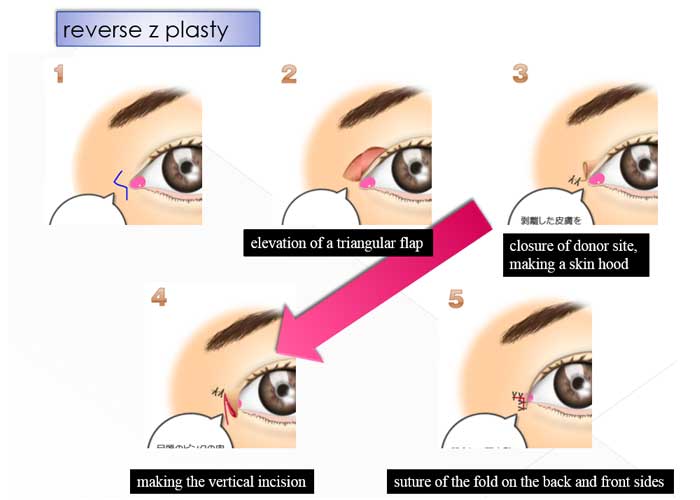
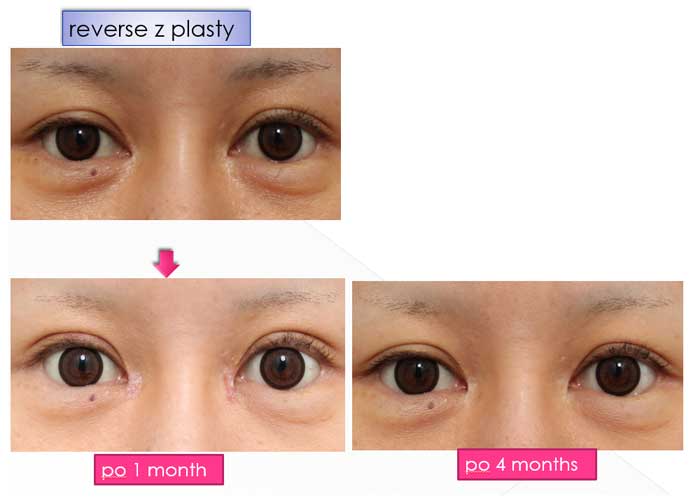
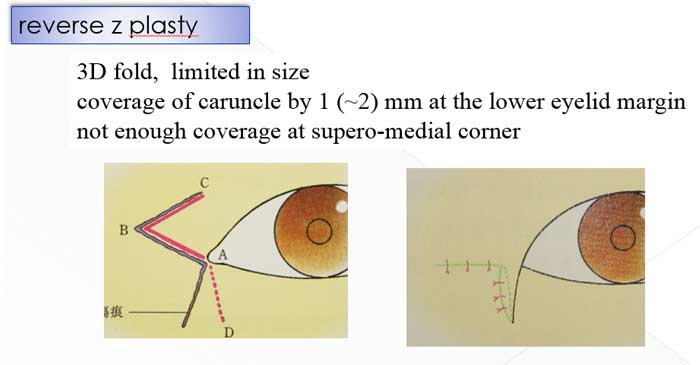
I use two different techniques. One is using Z plasty which is a reverse style of Z epicanthoplasty presented by Park JI.
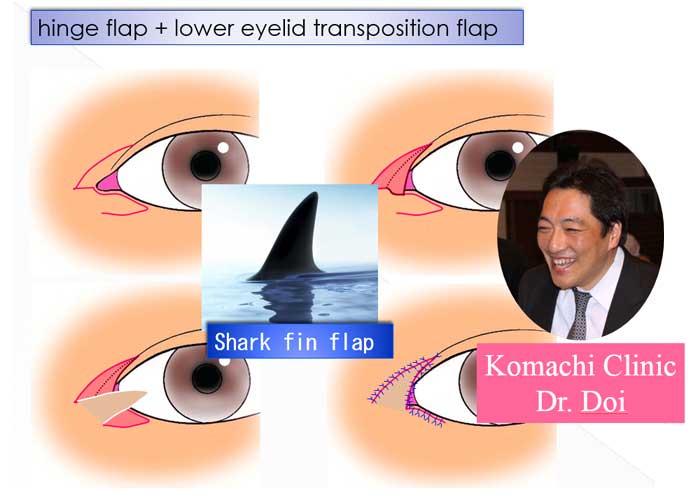
The other technique utilizes a hinge flap of medial skin and transposition flap from the lower eyelid; this was presented by Japanese plastic surgeon, Dr. Doi.
Z plasty technique creates an epicanthal fold which is limited in size.
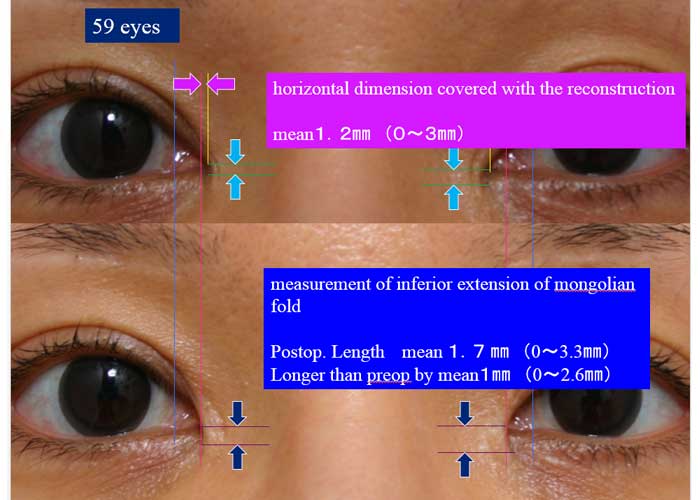
I use Z plasty for the patients who request coverage of the exposed caruncle by 1 mm.
For those require larger coverage of caruncle, I use transposition flap since this technique can provide larger tissue to the epicanthal region.
I had an experience of partial flap loss in transposition technique.
It was probably due to jeopardized blood supply to the flap which was elevated based on the scar from the previous epicanthoplasty operation.
I have currently applied delay procedure if the scar crosses the flap.
The surgical technique and clinical outcomes are shown in detail.
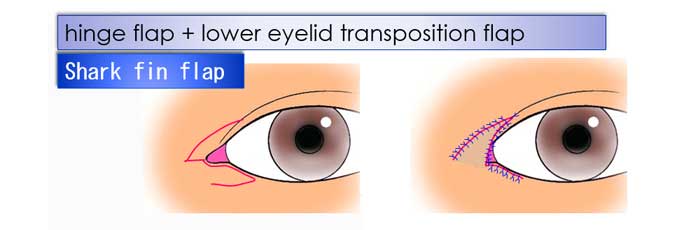
3D fold, large size
coverage of caruncle by 2~3 mm at the lower eyelid margin round curve at the infero-medial corner