韓国美容外科アカデミー鼻の整形外科研修コース part 1
Live surgery:
correction of bulbous tip, septal extension graft, alar reduction
A patient and a meeting

The explanation of operation contents

The operation end

1 correction of bulbous tip; management of cartilage frame
Keizo Fukuta, M.D.
Verite clinic, Tokyo Japan
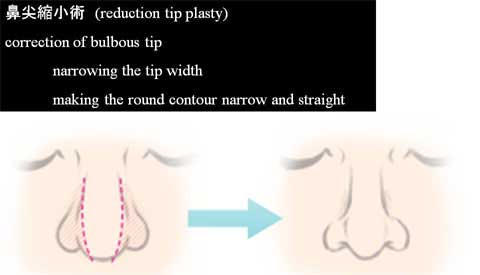
The request for tip correction is narrowing the tip width, reduction of the tip size, sharpening the round tip contour, increase of tip projection and reduction of nostril show.
We, rhinoplasty surgeons, usually focus on the nasal shape in the profile.
What the patients are concerned with is the front view of the nasal shape.
Many patients ask for making a broad and round contour of the nasal tip in the front view.
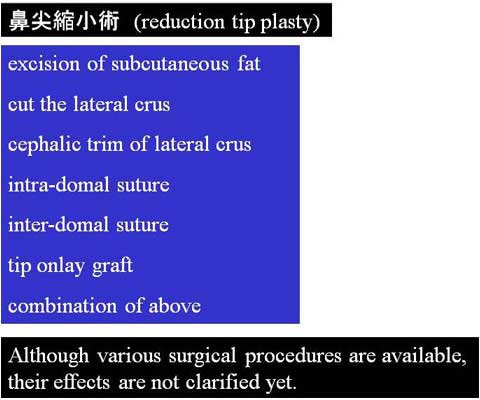
鼻尖縮小術(Reduction tip plasty) is a popular procedure for Japanese rhinop;lasty.
There are various surgical techniques, such as excision of subcutaneous fat, cutting the lateral crus, cephalic trim of the lateral crus, intra-domal suture, inter-domal suture, tip onlay cartilage graft and combination of these procedures.
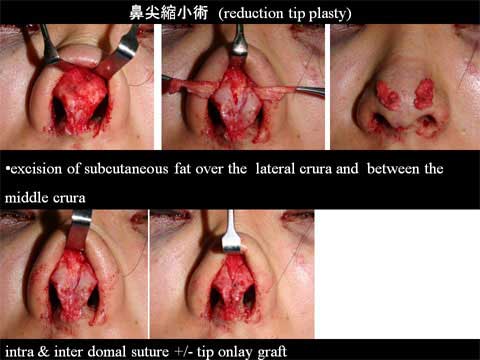
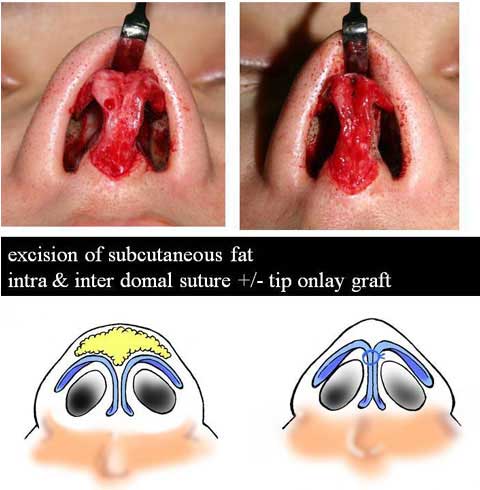
The operative techniques I used for reduction tip plasty were excision of subcutaneous fat overt he lateral crura and between the middle crura and inter-domal suture.
Onlay graft of ear cartilage was combined in many, not all, cases, depending on the tip projection.




My experiences showed that these combined procedure made very subtle change on the front view.
Although majority of the patients appreciated improvement, some of them were disappointed with the result.
A few patients present with wide domal area due to wide separation of bilateral middle crura, which is not common in Oriental.
Therefore the approximation of bilateral alar cartilages at domal region is not effective to correct bulbous tip.
The broadest part of round tip contour lies at the level of supratip in most of bulbous tip patients.
The broadest portion is far above the domal area and between upper 1/3 and upper 1/2 of the lateral crus in most of cases.
The lateral crus of the bulbous tip patient has convex surface on the skin side.
Some cases haves the latera crus, which is flat or even concave on the skin side.


It is therefore important to approximate the bilateral lateral crura from the domal area to upper 1/2 or upper 1/3 along the cephalic margin.
The suture will bring the bilateral lateral crura closer to each other and convert the convex surface of the crus to flat or concave surface.
Care must be taken that the sutures should not penetrate the mucosa or expose to the endo-nasal cavity.
The onlay carilage graft (shield graft) from the ear will be used depending on the requested tip projection.
Of course, as long as a patient accept the open rhinoplasty, it is always preferable.



I usually perform this procedure with endo-nasal approach.
For the close approach, I use bilateral infra-cartilagenous incision with medial extension along the columella down to the colummela base (foot plate).
This 10 mm extension of incision provides a great mobility of alar cartilage, making it possible to deliver the entire alar cartilage out of each nostril.
A lower 1/2 to 2/3 of cephalic margin of the bilateral lateral crura can be delivered through one nostril and approximation can be performed under direct vision.



The approximation of bilateral lateral crura along the cephalic margin was found effective to make the round tip contour narrow and smart.
 検索
検索