
第12回国際整鼻術ワークショップ、韓国、ソウル 2008/11/29-30
■ Anchoring of capsuropalpebral fascia to make a round shape lower eyelid
The Oriental people have the Mongolian slant of the orbital fissure. The lateral canthus is vertically higher in position when compared with the medial canthus.
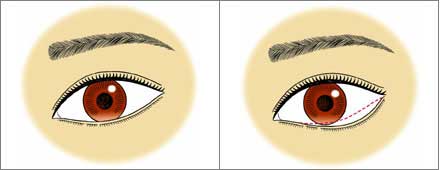
Many of the Oriental eyes have a fairly straight line or minimally curved line with inferior convexity of the lower eyelid margin.(fig 01) Some have a more curved line with downward convexity in the lateral portion of the lower eyelid.(fig 02) Some have round curve with natural lower scleral show.(fig03)

There are requests, although it is not very common, to make the lower eyelid margin lower.
The patients’ expectation is to make eye look larger and rounder from this morphological change. The popular request among them is lower the eyelid margin in the lateral portion, lateral to the cornea and to keep the lateral canthus in the position of Mongolian slant.(fig. 04,05)
The postoperative lowermost point of the lower eyelid margin could be at the midpupil line, lateral margin of the cornea, or further lateral to the cornear.
This has be determined preoperatively according to each patient’s request and marked on the lower eyelid skin.
Sample:
the lowermost point at midpupil,
the lowermost point at lateral limb 
the lowermost point lateral to the lateral limb 
The operation is performed with transconjunctival approach. (fig.14) An incision at the lower margin of the tarsus of the lower eyelid extends from the lateral corner to the medial corner.
Although this incision can be shorter medially, a long one provides us with wide exposure and good anatomical orientation.
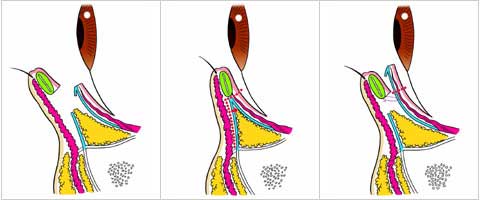
The dissection beneath the orbicularis oculi muscle is carried out to expose the orbital septum overlying the bulge of the central and lateral compartments of the orbital fat.(fig.09)
The orbital septum of the lower eyelid starts from the inferior orbital rim and extends superiorly close to the lower margin of the tarsus until it rolls backward to connect the capsuropalpebral fascia. The septum is incised horizontally near the upper margin.
The superior side of the incised septum is flipped up, which discloses the direct continuity of the septum and capsuropalpebral fascia. The downward retraction of the inferior side of the septum exposes the orbital fat pad.(fig.10,15)
The orbital fat can be excised to correct the baggy eyelid if it is indicated. The advancement of the capsuropalpebral fascia is performed at the planned postoperative lowermost point.
6-0 nylon suture is passed through the capsuropalpebral fascia at 10 mm below its upper margin, and then passed through the lower margin of the tarsus. (fig.11, 16)
The suture is temporally tied and the amount of lowering and shape of the eyelid margin is checked. (fig 12)
If the inferior traction is not enough, the tarsus is sutured to the further lower position on the capsuropalpebral fascia. Additional one or two sutures are usually required to achieve a round curved line of the eyelid margin.
The excess mucosa and capsuropalpebral fascia are excised by about 5 mm at the planned lowest point.(fig. 13) The mucosa is closed with 6-0 monocryl suture without repair of the septum.



This procedure shortened the posterior lamella of the lower eyelid, thereby creating an excess of the anterior lamella. The excess of the skin and orbicularis muscle produced has never developed the sagging or increased wrinkles of the lower eyelid.
The bulging of the pretarsal portion of the eyelid has been enhanced in some cases. The entropion with irritation of eye globe with eyelash has developed in about 10 % of cases.
It occurred in those who had had subclinical entropion preoperatively or those who underwent greater lowering of the eyelid particularly below the cornea. The entropion required the surgical correction with subcilial skin excision.
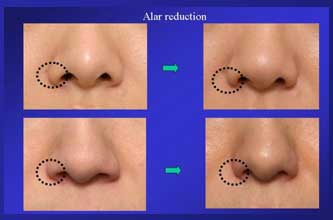
■ Alar reduction : surgical planning based on the nostril shape
Terminology of anatomy used in alar reduction surgery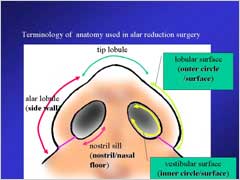
● design of alar reduction
– Selection of excision site (side wall or nasal floor)
● video presentation of operative technique
– Side wall excision with bunching suture
– Nasal floor excision with bilateral dermo-muscular flap
● demonstration of clinical cases
● documentation of change in alar and nostril shape following alar reduction
: design of alar reduction:
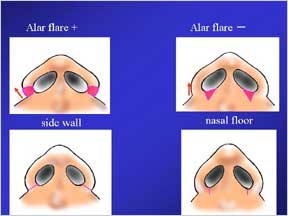
It is important to select the excision site (either side wall or nasal floor or both) according to the nostril shape (where the excess tissue exists)
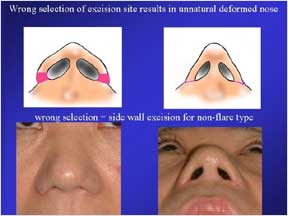
Wrong selection of excision site results in unnatural deformed nose such as side wall excision for non-flare type
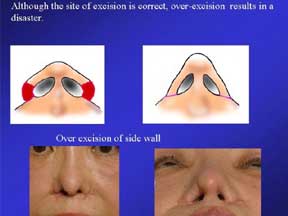
Although the site of excision is correct, over-excision results in a disaster. A sample of overexcision of side wall
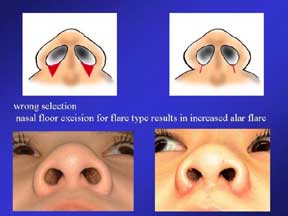
: wrong selection; nasal floor excision for flare type results in increased alar flare
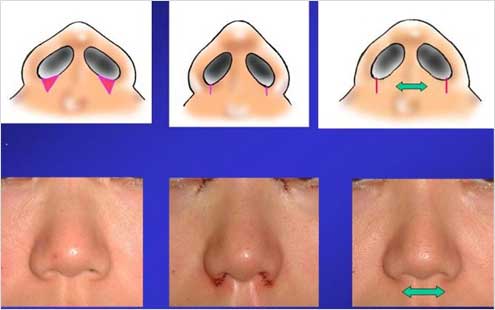
Excision of side wall is a treatment of choice for alar flare
In the majority of cases, the excision of the inner surface should be much smaller than the outer surface of the nostril to avoid a deformed nostril such as notch at the corner or too narrow nostril. A careful design of the tissue to be excised is a key for success.
The use of bunching suture between the bilateral alar lobule is helpful for further reduction of the alar width; however, bunching suture should be tied under small tension, making minimal squeeze like 2 or 3 mm of alar base width because overwhelming bunching not only creates an unnatural appearance in early postoperative stage but also develops fast relapse.
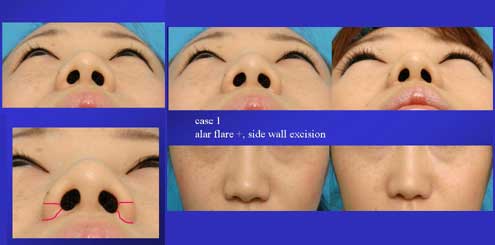
clinical case 1; Excision of side wall
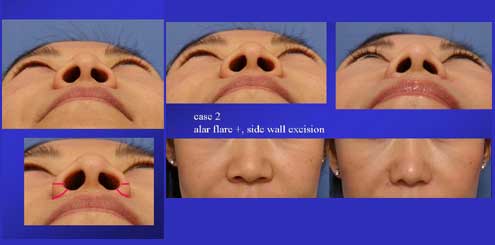
clinical case 2; Excision of side wall

clinical case 3; excison of outer surface of side wall
Excision of floor is a treatment of choice in a case with non flare alar.
The stretching of the central flap will make the surgery ineffective; therefore the maneuver to prevent the stretching of the central portion is essential.
The use of bilateral dermo- muscular flaps made of the tissue excised in the floor provide more predictable outcome.
The bilateral flaps are passed across the central portion through the subcutaneous tunnel and sutured to the contralateral flap.
stretch of central flap after nasal floor excision

clinical case 4; excison of nasal floor with bilateral dermo-muscular flap

clinical case 5; excison of nasal floor with bilateral dermo-muscular flap

clinical case 6; Excision of the nasal floor and the outer surface of side wall
effect of alar reduction on nasal shape
● reduction of alar width
● Shortening and caudal rotation of lateral nostril rim
● Reduction of lateral half of nasal hall in the front view

; Excision of side wall + Septal elongation
In summary
● Alar reduction procedure reduces alar width, makes the shortening and downward rotation of the lateral nostril rim and reduces lateral half of nasal hall in the front view.
● Alar reduction may enhances of columella retrusion; therefore the septal elongation with or without composite graft to the nostril rim should be taken into consideration.